If you’re reading this, it means that some of my work has sparked your curiosity about me – who the heck is this guy 😀? I’ve already written about me a couple of years ago here, but that information is outdated, so here’s an updated version. Here you can find out more about my past, present, and future.
Past: this is how I got into longevity
I was born in Romania, lived there until I was 18, and then moved to France, to study at “Classe Prépa” Louis-le-Grand and then to “Ecole Polytechnique“ and “Télécom Paristech”.
While being a student, I loved science, especially programming, physics, mathematics and entrepreneurship. This drove me to a career of more than 20 years as a startup entrepreneur in the tech space, during which I sold 2 startups. It has been a bumpy but exciting adventure, one I lived by always pushing myself beyond the limits.
When my last startup was acquired by a big US corporation, I was 40, and I reached the Holy Grail of financial independence. I discovered that by western standards, an individual will live up to 65 in (relatively) good health, and then yet 15 years suffering from chronic diseases. I only had 25 years to live in good health. Life is so beautiful, so many things to do, and so little time…
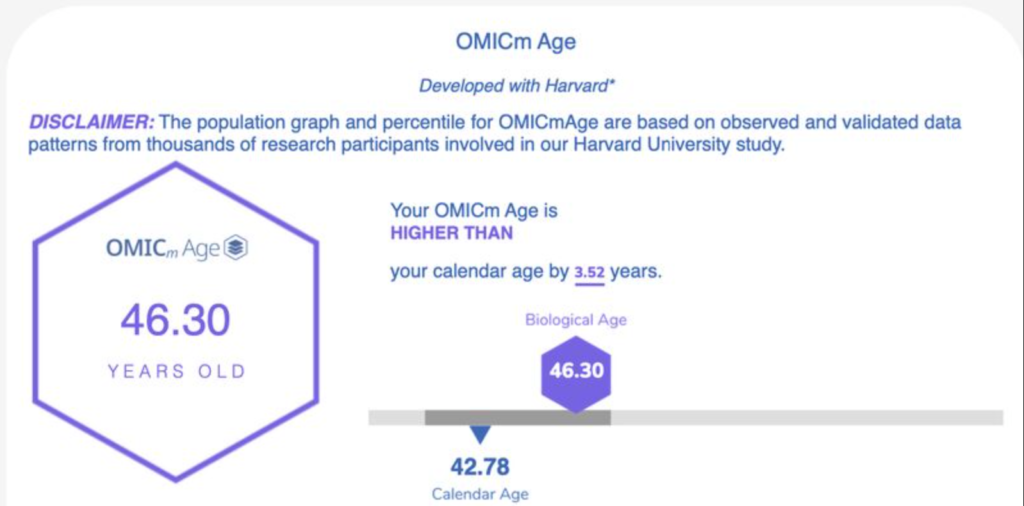
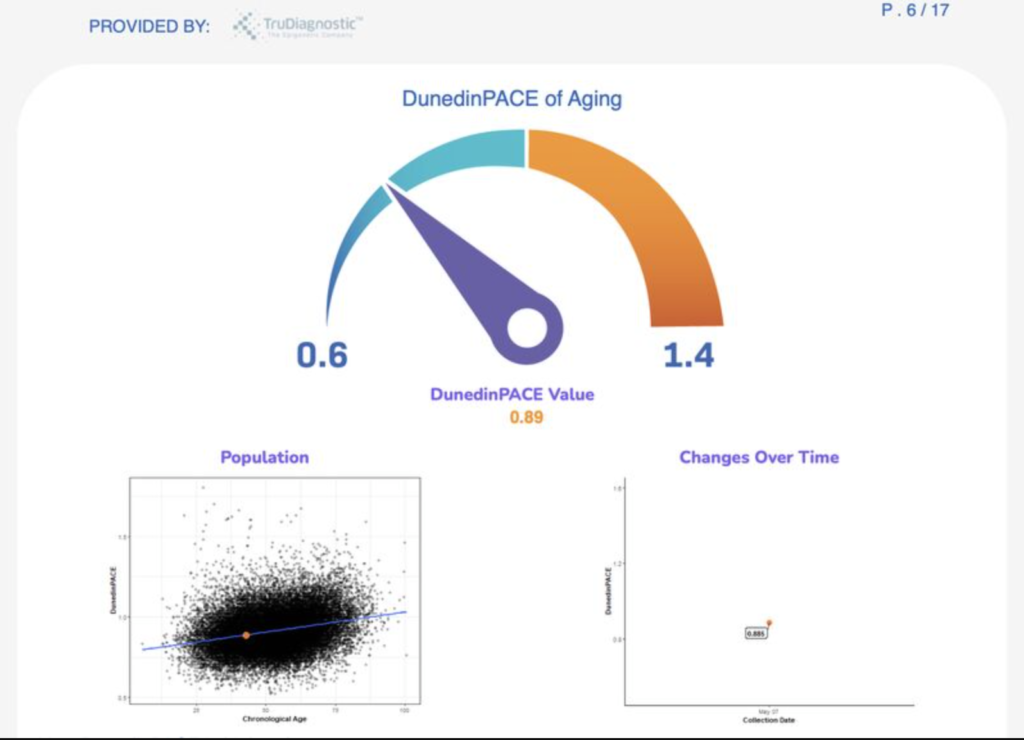
Although in apparently good health, with no pain, symptoms or signs, I have discovered that my health was a mess: I was prediabetic, I was suffering from chronic stress, and the overall body inflammation was equivalent to the one of a 72 years old individual. This was an incredibly powerful wake up call for me.
I decided that my life mission, what would be most aligned with my values as aspirations, is to help Humanity defeat aging before 2060. In the worst case scenario, I’ll spend the next 40 years of my life working on fascinating projects (life extension) with fascinating people. And in the best case scenario, if we execute the action plan well enough, we will all be rewarded with living longer and healthier.
This seemed the best option at hand for the 2nd part of my life. This is how I got into longevity.
Present: creating an ecosystem to help people live longer and healthier
After exploring the longevity space, I have discovered that:
-Humanity is on the brink of disrupting life as we know it. Thanks to major scientific and technological breakthroughs, we’re the first generation of Humans for whom defeating aging is an ambitious yet attainable goal, provided we put in the right amount of resources
-Longevity is the best investment opportunity of our times. The research going on, some of it very close to market deployment, is absolutely astounding. Therefore, working in longevity is not only the best path to living longer and healthier, but also a tremendous business and investment opportunity
-the best way to get to Longevity Escape Velocity, and access to future life extension technologies, is to have a short term / long term strategy: in the short term, use state of the art preventative medicine, and in the longer term, put resources into promising R&D and startups working on futuristic technologies.
This is what brought me to work on creating an whole longevity ecosystem, covering the whole short term / long term spectrum of the action plan :
– Ikare helps people live 100+ years in good health, thanks to the last breakthroughs in preventative medicine
– the “2060 Longevity Forum” federates the whole longevity community once a year, in the South of France, one of the most culturally sophisticated, longevity friendly and beautiful places on Earth
– the “2060 Longevity Club” is a community of investors who invest in high-potential longevity startups.
Future: defeating aging before 2060
As years pass by, the scientific progress and the demographic tsunami (less young people, more old people) are pushing governments to become aware of longevity and its huge potential.
This creates a wonderful opportunity to accelerate the pace of research, and bring Humanity to a tipping point where governments will massively invest in longevity, until we defeat Aging. Investing 1% of the global GDP in longevity is a great goal to pursue in this regard.
This will probably take decades, careful planning, and numerous public and political advocacy campaigns.
The 2060 Foundation statement of purpose is to make that happen. I’m not here for quick superficial wins, I’m here to pursue Humanity’s most audacious and long term aspiration: Defeating Aging.